
General points
The risk factors for road accidents are well-known and detailed in annual road safety reports.
Most of these reports conclude that the driver is responsible in more than 90% of cases.1
The French Government’s road safety data is some of the most comprehensive data available online.
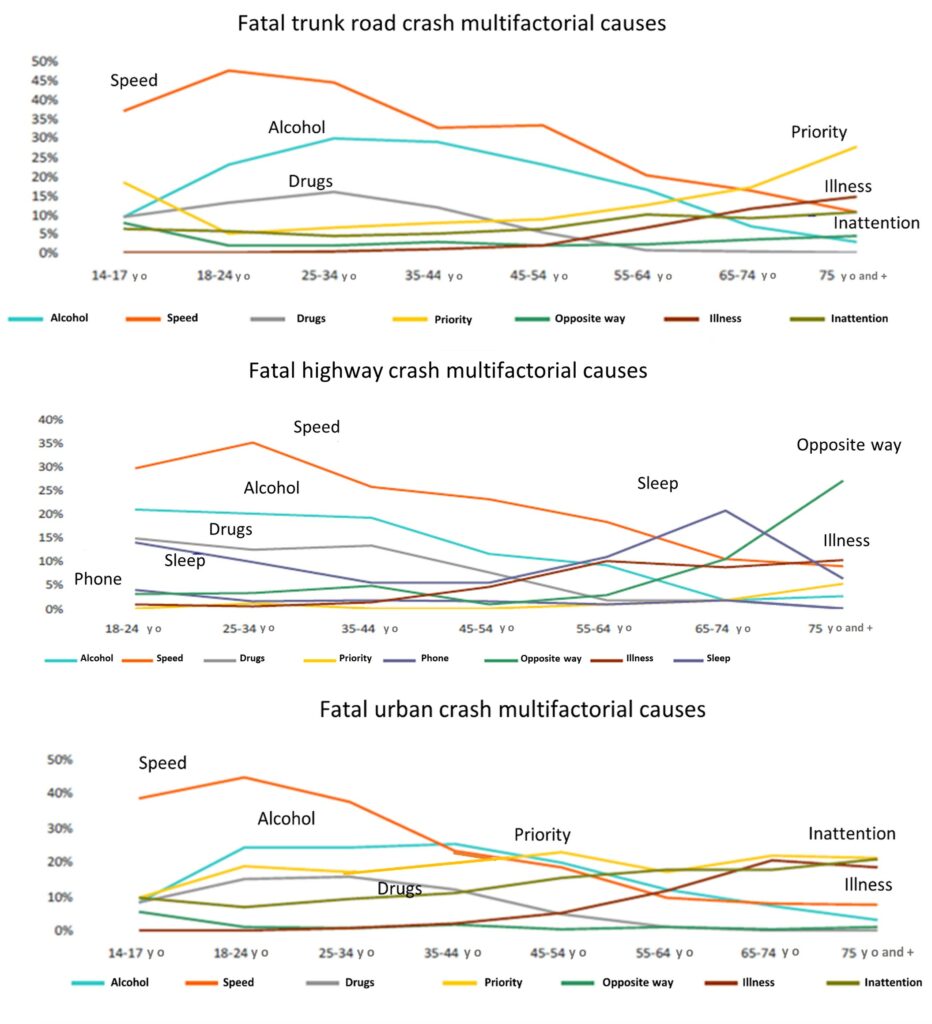
According to their data: speeding, alcohol consumption and not following road-priority rules were the highest factors in fatal vehicular accidents (Table 1). Discomfort and Drowsiness rank 6th and 7th respectively but, when adjusted for age, are more frequently reported by those above 55 years, regardless of other factors (Figures 1, 2 and 3).
The risk factors for road accidents are well-known and detailed in annual road safety reports.
Most of these reports conclude that the driver is responsible in more than 90% of cases.1
The French Government’s road safety data is some of the most comprehensive data available online.
According to their data: speeding, alcohol consumption and not following road-priority rules were the highest factors in fatal vehicular accidents (Table 1). Discomfort and Drowsiness rank 6th and 7th respectively but, when adjusted for age, are more frequently reported by those above 55 years, regardless of other factors (Figures 1, 2 and 3).

Disease on road
Understanding the methodology used is important to analyze these results.
Accidentology is a rigorous discipline which scientifically studies the causes of accidents by using different approaches.
The most known are the “fault tree method” (Anglo-Saxon model) and the “cause tree method” (French model).
Each branch of the tree is designed with objective, reliable and measurable facts present at the time of the accident and assembled to schematize the cascade of causal events.
Blood alcohol level, speed, weather, or road conditions are all objective evidences: the pre-crash driver’s physical condition is not considered an objective fact because it is based on the report of witnesses or the injured victims.
If those involved are still in a position to respond their memories may be altered by a state of shock, head trauma or a prolonged coma.
Guilt may also affect testimony by incentivizing downplaying a known health problem. Distraction, falling asleep or other worrying behaviors are sometimes the result of an unknown pathological condition (hypoglycemia, sleep apnea…).
Therefore, a larger panel of road crashes could be concerned by medical conditions and 10% of unexplained accidents could find their origin there. Conversely, medical events behind the wheel do not always lead to accidents when patients manage to stop their vehicles in time.
In conclusion, assessing the impact of a patient’s health on driving is not a simple task as adverse effects are not synonymous with accidents.
Understanding the methodology used is important to analyze these results.
Accidentology is a rigorous discipline which scientifically studies the causes of accidents by using different approaches.
The most known are the “fault tree method” (Anglo-Saxon model) and the “cause tree method” (French model).
Each branch of the tree is designed with objective, reliable and measurable facts present at the time of the accident and assembled to schematize the cascade of causal events.
Blood alcohol level, speed, weather, or road conditions are all objective evidences: the pre-crash driver’s physical condition is not considered an objective fact because it is based on the report of witnesses or the injured victims.
If those involved are still in a position to respond their memories may be altered by a state of shock, head trauma or a prolonged coma.
Guilt may also affect testimony by incentivizing downplaying a known health problem. Distraction, falling asleep or other worrying behaviors are sometimes the result of an unknown pathological condition (hypoglycemia, sleep apnea…).
Therefore, a larger panel of road crashes could be concerned by medical conditions and 10% of unexplained accidents could find their origin there. Conversely, medical events behind the wheel do not always lead to accidents when patients manage to stop their vehicles in time.
In conclusion, assessing the impact of a patient’s health on driving is not a simple task as adverse effects are not synonymous with accidents.
Acute illness and driving
Road use can generally be divided into several categories:
– Casual travel involving, intermittent, mixed short and long-distance travel with extra professional travel.
– Short-distance professional road travel involving repeated journeys in areas of heavy urban or semi-urban traffic (taxi or public transport drivers, delivery drivers, etc.).
– Long-distance professional road travel involving extended national road or motorway journeys (lorry driver).
If driving does not significantly increase illness among occasional drivers, the prevalence of certain pathologies raises with the frequency and type of the vehicle use.
Previous studies suggest that it is uncommon for the first manifestation of a serious condition to occur while driving, with an estimated incidence rate of 1-3%.2-4
The Canadian Cardiovascular Society (CCS Consensus Conference (1996)) proposes that the risk of a subject with a serious condition injuring a third party in an accident is approximated by the following equation:
RH = TD × V × SCI × Ac
Where RH = Risk of Harm to another user
TD = Time of driven
V= Type of vehicle
SCI= risk of sudden cardiac incapacity
Ac= risk of injury or death caused by the accident
It follows that the risk of crash appears very low for a casual driver without prior medical history or symptoms.
The possible dangers are different for people with a medical condition or professional drivers due to driving time and the vehicle type. The increase in calculated risk justifies regular health checks and driving restrictions in many countries.
Road use can generally be divided into several categories:
– Casual travel involving, intermittent, mixed short and long-distance travel with extra professional travel.
– Short-distance professional road travel involving repeated journeys in areas of heavy urban or semi-urban traffic (taxi or public transport drivers, delivery drivers, etc.).
– Long-distance professional road travel involving extended national road or motorway journeys (lorry driver).
If driving does not significantly increase illness among occasional drivers, the prevalence of certain pathologies raises with the frequency and type of the vehicle use.
Previous studies suggest that it is uncommon for the first manifestation of a serious condition to occur while driving, with an estimated incidence rate of 1-3%.2-4
The Canadian Cardiovascular Society (CCS Consensus Conference (1996)) proposes that the risk of a subject with a serious condition injuring a third party in an accident is approximated by the following equation:
RH = TD × V × SCI × Ac
Where RH = Risk of Harm to another user
TD = Time of driven
V= Type of vehicle
SCI= risk of sudden cardiac incapacity
Ac= risk of injury or death caused by the accident
It follows that the risk of crash appears very low for a casual driver without prior medical history or symptoms.
The possible dangers are different for people with a medical condition or professional drivers due to driving time and the vehicle type. The increase in calculated risk justifies regular health checks and driving restrictions in many countries.
References
- Stork AD, van Haeften TW, Veneman TF. Diabetes and driving: Desired data, research methods and their pitfalls, current knowledge, and future research. Diabetes Care 2006;29:1942-9.
- Petch MC. Driving and heart disease. Eur Heart J 1998;19:1165-77.
- Herner B, Smedby B, Ysander L. Sudden illness as a cause of motor-vehicle accidents. Br J Ind Med 1966;23:37-41.
- Norman LG. The health of bus drivers: a study in London transport. Lancet 1958;2:807-12.